Thirteen years ago, when Babalwa Mbono was eight months pregnant with her second child, she went to her clinic in Cape Town, South Africa, to have a routine HIV test.

“I went with confidence because my first child was negative and I was negative then,” she says. When the test came back positive, Mbono couldn’t believe it. “When the counsellor who tested me showed me the results I thought, ‘you’re joking!’ I even asked her if she was sure.”
Mbono left the clinic in a daze and went home to reflect on the news, still in denial. She looked healthy and well, unlike her sister who had died three years previously from Aids-related tuberculosis. “For me, [the result] was something that was not real,” Mbono adds.
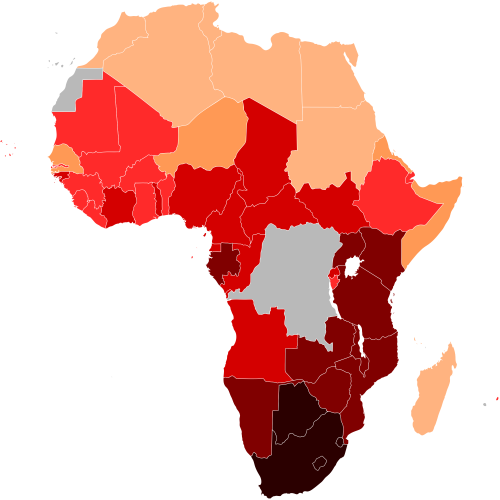
Nowadays many people in South Africa know about HIV. The country has the biggest and most high-profile epidemic in the world, with an estimated 7 million people living with the condition, according to UNAids figures. But in 2003 it was not a big topic, and discussions usually revolved around death, says Mbono. The fear of what having HIV might mean for her unborn child started to creep in, and she worried that she would not live long enough to care for a baby who might be infected.
When Mbono found out that she had HIV, South Africa’s government was still deciding whether to make antiretroviral treatment (ARVs) available to all, despite a third of pregnant women testing positive. Today, 48% of infected South African adults are on ARVs.
Back at the clinic, Mbono was linked up to a mentor mother through Johnson & Johnson’s mothers2mothers (M2M) programme. The scheme started in 2001 and has helped 1.4 million HIV-positive mothers in nine sub-Saharan African countries. It currently operates in Kenya, South Africa, Malawi, Lesotho, Uganda, Swaziland and Zambia – seven countries where it has virtually eliminated mother-to-child transmission (MTCT) among its patients, with a 2.1% transmission rate (the UN classifies virtual elimination as less than 5%).
Mbono’s HIV-positive mentor allayed her fears about death and her anger towards her husband, whom she blamed for giving her HIV after he tested positive with a much higher viral load. Through M2M, Mbono learned about taking ARVs to reduce the risk of MTCT in the womb and during breastfeeding, and about how to change her lifestyle to live a long and happy life with her children.
Last year, South Africa was one of six priority countries (all in sub-Saharan Africa) to meet a Global Plan target of reducing MTCT by 90%, with 95% of pregnant women with HIV on ARVs and an 84% reduction in new HIV infections among children.
Over the past year, Cuba, Belarus, Armenia and Thailand – non-priority countries – managed to eliminate MTCT altogether. In South Africa, mother-to-child transmission of HIV has fallen to 3.5%, putting the country within reach of eliminating paediatric infections, although maternal mortality remains high.
The M2M programme “makes the person feel supported”, Mbono says. “It’s a sisterhood, and it makes you feel like you have a family to cry on.” Through counselling, which helps to breaks down the stigma still attached to HIV/Aids in South Africa despite its high prevalence, Mbono also found the courage to confide in her parents and siblings.
And six months ago, she decided to disclose her HIV status to her daughter Anathi, who had just turned 13. “It really felt shocking,” says Anathi, who feared that there would be no one to look after her seven-year-old brother, who was born HIV negative. “I was afraid that she would leave us.”
Mbono reassured her daughter that she had tested negative when she was 18 months old, but Anathi decided to go alone to the clinic and be tested anyway, where she also accessed free counselling from health workers.
“I was so, so scared, but eventually they just sat with me and told me to not freak out and to not think negative things about my mum,” Anathi says. Over the two days she waited for her results, she spent time with her mother and learned more about M2M, even reading her mentoring books.
Mbono’s experience with M2M made her give up unhealthy habits, such as not eating properly and drinking alcohol, and inspired her to become a mentor mother in 2003. “The [programme] gave me the strength to go out there and tell people about HIV and correct the mistakes that people are making and [that] I also made when I didn’t have any information.”
She has gone from counselling others on HIV/Aids and family planning, to training other mentors and seeing them become nurses, social workers and students.
“What makes me most happy [is] when I see a woman who had broken up in pieces when she was told about HIV … and when you see her on the next visit she is much better than the day she left.”
Some 95% of babies in M2M’s South Africa programme test negative for HIV at 18 months, and that also makes Mbono proud. “That makes me feel that I’ve done my job, because 18 months is a long time for the mother to be supported and to be educated. There are so many challenges that they come across, and we are there [for them].”
Anathi set up a counselling group at school to discuss HIV and sex with 18 girls and five teachers, as well as a drama group to perform plays to parents and pupils that discuss staying HIV negative and breaking down stigma.
“Most people don’t talk about it … Young people are not getting enough information about HIV,” she says. Anathi has a friend who she says became a recluse after she found out she is positive, and she knows two girls who have gone off the rails since their mothers recently died of Aids.
But for Anathi, dealing with her mother’s HIV has made them stronger and brought them closer together.
She still worries about how well her mother has slept or eaten when they are apart, even though learning about ARVs has lessened her fears of her mother falling ill and not recovering. “I just worry too much and I call,” she says. “She is like my daughter.”
Thanks for reading, let us know what you think in the comments below, or you can find us on Facebook, Twitter or Instagram!